The Menstrual Cycle: Putting it all together
Part 3 of the Menstrual cycle series
MENSTRUAL CYCLE
Lara El-Hoss, MAN, APRN, CNM
1/29/20266 min read
Welcome to Part 3 of the Menstrual Cycle Series:
Let’s take a ride on the menstrual cycle roller coaster from start to finish. Before we do, let’s recap what we learned in parts 1 and 2:
Structures:
Hypothalamus: Director and coordinator, sends messages to the pituitary gland, receives feedback messages.
Pituitary: Receives messages from the Hypothalamus, sends messages to the ovaries. Receives feedback messages from the ovaries.
Ovaries: Receives messages from the pituitary. Send feedback messages to the Pituitary and Hypothalamus.
Uterus: Receives messages.
Hormones:
GnRH: A releasing hormone sent by the Hypothalamus to the pituitary.
Follicle-stimulating hormone (FSH): Released by the anterior pituitary after receiving messaging from GnRH. Tells the ovaries to grow their egg follicles.
Luteinizing hormone (LH): Released by the anterior pituitary to stimulate release of an egg, aka “ovulation”.
Estrogen: Steroid hormone. Produced as ovarian follicles grow and mature. Helps uterine lining to “proliferate”, ie grow.
Inhibin: Chemical messenger that tells the pituitary to slow down on FSH when follicles are mature and estrogen is high enough.
Progesterone: Literally meaning “Pro-gestation”. Rising levels produced by the follicle from which an egg emerged work on the uterine lining to create a coiled/twisted and “secretory” environment-think of it as becoming more cushy and nutritious. Estrogen grows the uterine lining, progesterone adds the finishing touches that help sustain an implanted embryo.
A few things to remember–this is a cycle based on feedback loops, not a linear process happening in isolation. But for the purposes of education, I have tried to simplify my explanation in order to get across the most important concepts. One important detail is the cycles. We hear it referred to as the menstrual cycle, but it’s really more like 2 cycles–what’s happening in the ovaries, and what’s happening in the uterus simultaneously.
Okay, let’s take a ride.
Days 1-7 in the Endometrial/Uterine Cycle: The first day of the menstrual period, or menses, is the first day of “red” blood–this is what you want to count as your Day 1. Do not count your first day or so of brown spotting. When you see red blood, mark that day on your calendar or app.
In the uterus: The uterine lining is weak, shrunken, and atrophied due to a drop in estrogen and progesterone (remember, their rise grows and readies the lining for implantation). The lining is shed through menses on days 1-7.
Okay, we’ve established what the uterus is doing on Days 1-7 (days are approximate/averages-cycles may be longer or shorter). The endometrial lining is sloughing off, getting rid of dead tissue and blood. We’ll swing back around to days 7-14 later.
We also know that estrogen and progesterone are low during this time. The hypothalamus gets the message that we are not pregnant, and estrogen and progesterone have dropped. As a result, it does what we discussed in previous posts-it releases GnRH, sending a message to the pituitary to start producing more FSH and LH. FSH and LH act on the ovaries, so let’s catch up with the ovarian cycle.
Days 1-14 in the Ovarian cycle: The first phase of the ovarian cycle in days 1-14 is the Follicular phase. Remember our follicles in the ovaries? In the follicular phase, FSH (follicle-stimulating) is being released by the pituitary and slowly rising, sending a message to the ovaries to grow and mature some follicles in preparation for ovulation. This whole process starts when a period starts-the cycle is always going.
So, our follicles are maturing and continuing to grow, which causes estrogen to rise. The pituitary gets the message that estrogen is up, follicles are stimulated, we can slow down on the FSH. We have several maturing follicles, but we really only need one (except in cases of multiples), so a gladiator follicle emerges triumphant as the dominant follicle for that cycle. All the other follicles take a back seat while our gladiator follicle continues to produce estrogen. Once estrogen reaches its peak, the hypothalamus gets the message, and does its job again by increasing GnRH, telling the pituitary hey, time for the gladiator to enter the arena–send a surge of LH so that the follicle can release its egg and ovulation can occur. LH jumps up, and the gladiator egg is released from its follicle around day 14 and begins its wait for a sperm to fertilize it.
While our egg is waiting, let’s circle back around the uterus. What’s happening in the uterus days 7-14 leading up to ovulation? After menstruation ends, the uterus needs to be prepared for possible pregnancy. That means we have to grow the endometrial lining. Remember what helps grow the lining, and what has also been increasing since follicle-stimulating hormone was released? Estrogen! The steady rise in estrogen is thanks to our maturing ovarian follicles. It acts on the endometrial lining and helps it grow back again after menstruation, so that by day 14 when ovulation happens, the uterine lining is rebuilt.
Okay, we’re about half-way through the cycle. To recap:
Days 1-14:
Days 1-7 in the uterus: Estrogen & progesterone are down–we are not pregnant. The uterine lining cannot be sustained. It weakens, shrinks, and sheds its blood supply.
Days 1-7 in the ovaries: It’s the follicular phase! The hypothalamus gets the message that we are not pregnant. It sends out GnRH to the pituitary and tells it to get on with making more follicles in preparation for the next cycle. The pituitary releases FSH.
Days 7-14: The ovarian follicles begin producing estrogen as they grow and mature, with one gladiator follicle emerging triumphant and continuing to produce more estrogen. FSH production slows due to rising inhibin (“inhibits” FSH). Under the influence of estrogen, the uterine lining enters its “Proliferative” phase, growing and enlarging. Estrogen peaks, and the hypothalamus signals to the pituitary that it is time for LH to step up. LH surges, prompting the gladiator follicle to rupture and release an egg-Ovulation!
A word on the details of ovulation. I’ve simplified the cycle as a whole for education purposes, but for those interested from a fertility planning perspective, here are some tidbits:
Ovulation is not always on day 14. It varies based on cycle length, and can be influenced by many different factors. So how do we reliably pinpoint it?
Estrogen peak: Ovulation occurs 24-36 hours after this
Cervical mucus becomes increasingly copious, clear, and stretchy, like raw egg white.
Some may feel a little twinge or crampy on one side.
LH surge: Ovulation occurs 10-12 hours after this. This is what ovulation predictor kits test for.
Now, there are 2 tracks we can take. For our purposes right now, we are remaining on the non-pregnant track. We can take the pregnant track in an upcoming post.
Days 14-28: This is known as the Luteal Phase for our ovarian cycle, as it relates to LH (Luteinizing Hormone), and the “Corpus Luteum”. Remember, the corpus luteum is the follicle that has just released an egg-it still has an important job to do. It secretes progesterone, helping prepare the uterine lining for potential pregnancy. Estrogen has grown the lining, now progesterone helps make that lining nice and cushy by helping the blood vessels of the lining twist and spiral, while the glands also twist and turn. This is why this phase of the cycle for the uterus is called the secretory phase, and why progesterone is such an important part of maintaining pregnancy. The progesterone creates the ideal environment to nurture a developing embryo.
So what happens if we do not get pregnant? Roughly 7-8 days after ovulation, (day 21 ish), the corpus luteum has produced the maximum amount of progesterone that it can. Progesterone then begins to decline, the corpus luteum shrinks, and estrogen and its friend inhibin also decline. Remember, inhibin is the friend that tells our feedback loop that we don’t need more follicles. So when our hypothalamus gets the message about the decrease, it starts to produce more GnRH and increase FSH and LH again, because we are not pregnant, and we need to try again at the next cycle. That brings us back around to Day 1 of a new menses.
Whew! This ends Part 3 of the menstrual cycle series. It is a lot to process, but this is really helpful information, especially when it comes to understanding fertility tracking, pregnancy, menstrual mood changes, and what our bodies are doing throughout the cycle. If you have questions, please reach out, and tell me what else you’d like to learn about.
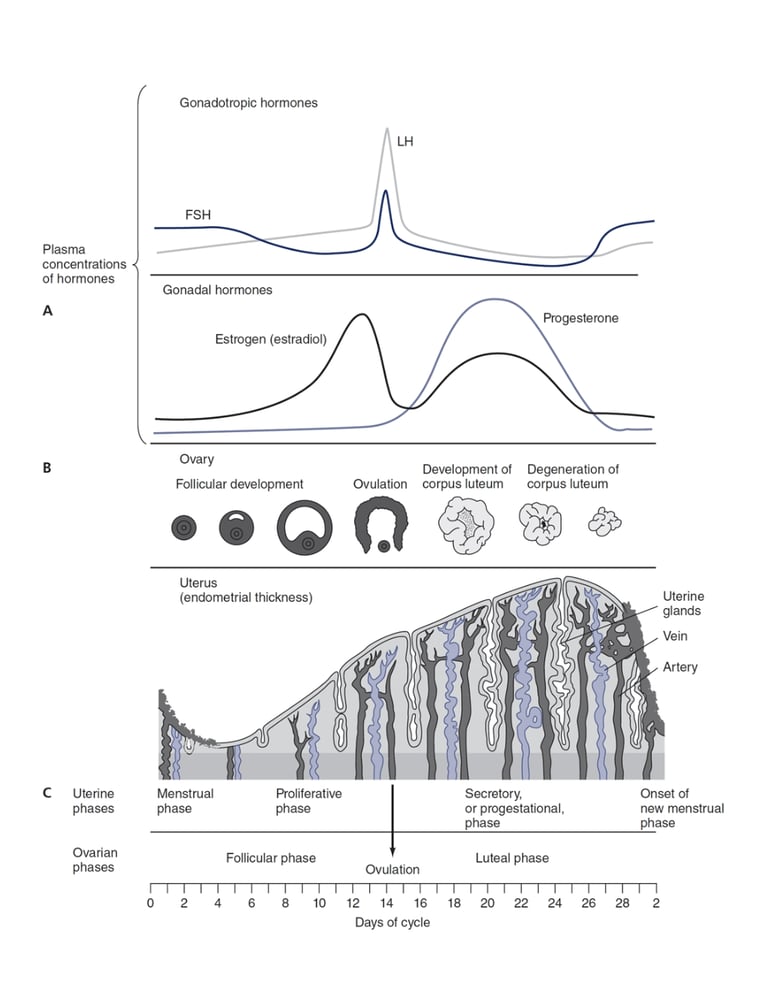
Below is a great representation of the menstrual cycle that illustrates what is happening in the ovaries and uterus in relationship to hormonal shifts.
Taken from the 7th Edition of Varney’s Midwifery, which reproduced it from: Chiras DD. Human Biology. 9th ed. Burlington, MA: Jones & Bartlett Learning; 2019.
Contact
Email:
(602) 430-4257
© 2025. All rights reserved.
Text me:
Instagram: